|
Overview
The arch of the foot is a very complex structure, consisting of multiple bones and ligaments. Most causes of arch pain are related to the anatomy of the arch and the types of physical activity that you perform. For example, a classic set up for arch pain is people who engage in lots of high impact exercise (such as running) while wearing a type of athletic shoe that does not properly support their type of foot arch. If you notice that the twinges of pain you have are most commonly associated with or immediately after exercise, you might want to visit a good athletic shoe store to make sure you are wearing the right kind of shoe. Another cause of arch pain is plantar fasciitis. The plantar fascia is a tough tissue structure that holds the bottom part of the arch in place. The fascia often becomes inflamed and sore, usually as a result of repetitive motion (for example, very common in those who stand on their feet for work). The pain is often noticeable first thing in the morning and worse with activity. In addition to wearing good arch supports and taking anti-inflammatory medications, stretching exercises are often a part of the treatment. You should see your primary care doctor to determine what is the best treatment for you.  Causes Sprains, strains, bruises, and fractures may be the result of a single stress or a combination of stresses to the foot. A blunt-force injury such as someone stepping on your foot may result not only in a bruise (contusion), but also in damage to the primary and secondary structures of the foot. Many of the muscles of the lower leg and foot attach on or near the arch. Injured or tight muscles may lead to incorrect biomechanics and in turn cause arch pain. Injury to the bones of the foot can be caused by a single blow or twist to the arch or also by repetitive trauma, which can result in a stress fracture. A sprain of the arch occurs when the ligaments which hold the bones together are overstretched and the fibers tear. The muscles of the foot may be strained by overstretching, overuse, overloading, bruising, or being cut by stepping on a sharp object. Arthritis of the arch joints may also occur if the foot is subjected to repetitive movements that stress the arch. Symptoms Repetitive exertive activity arch pain is usually sharp, and localized to a specific area, rather than the entire arch. Usually the pain occurs in the area just in front of the heel. It is present when first standing on the foot in the morning, but may decrease once you start walking around, but will, gradually becomes worse with continued walking or running. Swelling may be present. The pain subsides with rest, but stretching the arch while resting may cause the pain to return. Injury pain is constantly present, but worse when standing on the foot. This pain is localized to a specific area, but may radiate out from this area to the entire foot. The pain is sharp, and usually accompanied by swelling and occasionally "black and blue" discolorations. The pain due to the natural aging process is usually dull and aching, or stiff, and can be felt throughout the entire arch area, rather then in just one spot. This pain is present whenever weight bearing, and usually becomes worse with continued walking. The pain gradually subsides when resting, and usually does not return with stretching. Biomechanical defect pain is usually localized to a section of the arch, such as the inner, middle, outer, front, or back of the arch. This pain may be sharp or dull, but is always worse with continued walking. Diagnosis A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to "raise up on the tip toes" of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes. X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet, the symptomatic and asymptomatic - will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side. Non Surgical Treatment Arch pain can be treated with orthotics, inserts that have proper arch support to relieve the strain on the plantar fascia, mild stretching and anti-inflammatory medications. Orthotics will relieve most of the strain put onto the plantar fascia by supporting the band from underneath when pressure is applied. Tape can also be used in conjunction with orthotics to restrict movement and support the plantar fascia. Stretching should be used along with orthotics and continued long after the symptoms of arch pain are gone to prevent it from occurring again.  Surgical Treatment The main goal of surgery is to reduce pain and improve function. It may also reduce other injuries such as repeated ankle sprains and broken bones. Surgery may be considered if there is no relief with physical therapy, changes in shoewear and/or changes in activity. Some patients will also have tendon problems, ankle weakness and foot fractures. These patients may require other procedures to address related problems. If you have medical problems that make surgery unsafe, any infections or blood vessel disease, cavus foot surgery may not be appropriate. The surgical procedures involved with the correction of the cavus foot are varied. Theses may include correction of the bony deformity, ankle looseness and the muscle imbalances that cause the deformity. The goal is to provide a foot that evenly distributes weight along both inside and outside edges. A variety of incisions may be needed to perform the procedures related to the correction of the cavus foot. Prevention There are several things you can do to prevent pain on the bottom of the foot. Here are some tips to help you avoid this condition. Do simple stretches each day (See Plantar Fasciitis Exercises for a list of all exercises). Wear good shoes that fit properly and are appropriate for the activity you are participating in. Lose excess weight if possible. Build your stamina slowly, especially with new exercises. Rest and elevate your feet, whenever possible, keeping them at least twelve inches above your heart. Always follow your doctor?s instructions for treatment. Each day do a different activity. For example: one day ride your bike, and swim the next day. Stretching Exercises Ankle evert or strengthening. Lie on your side with your feet hanging off the end of your bed or a weight bench. Bend the toes of the foot that is closer to the ceiling slightly toward your head. This is the starting position. Now raise your toes toward the ceiling while keeping the rest of your leg stationary. Return to the starting position. Reps. 10-15. Now point your toes slightly away from your head. This is the starting position. Raise your toes toward the ceiling. Return to the starting position. Reps. 10-15. Ankle invertor strengthening. Same as above, but do the exercises with the foot that is closer to the floor. Dorsiflexor strengthening. Sit on a desk, table, or counter so that your feet don?t touch the ground. Let your feet dangle comfortably. Bend your foot upward as far as you can comfortably go. Do not let your foot pull inward or outward. Return to the starting position. Reps. 10-15. Overview 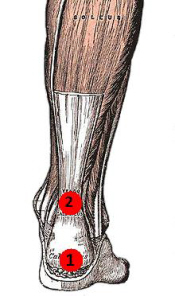 Achilles tendon ruptures commonly occur in athletic individuals in their 30s and 40s while performing activities that require sudden acceleration or changes in direction (ex. basketball, tennis, etc.). Patients usually describe a sharp pain in their heel region almost as if they were struck in the back of the leg. The diagnosis of an acute Achilles tendon rupture is made on clinical examination as x-rays will reveal the ankle bones to be normal. The Achilles is the largest and strongest tendon in the body. It is subject to 2-3 times body weight during normal walking so regaining normal Achilles tendon function is critical. Achilles tendon ruptures can be successfully treated non-operatively, or operatively, but they must be treated. Surgical treatment leads to a faster recovery and a lower rate of re-rupture. However, surgery can be associated with very serious complications such as an infection or wound healing problems. For this reason non-operative treatment may be preferable in many individuals, especially those patients with diabetes, vascular disease, and those who are long-term smokers. Achilles tendon ruptures commonly occur in athletic individuals in their 30s and 40s while performing activities that require sudden acceleration or changes in direction (ex. basketball, tennis, etc.). Patients usually describe a sharp pain in their heel region almost as if they were struck in the back of the leg. The diagnosis of an acute Achilles tendon rupture is made on clinical examination as x-rays will reveal the ankle bones to be normal. The Achilles is the largest and strongest tendon in the body. It is subject to 2-3 times body weight during normal walking so regaining normal Achilles tendon function is critical. Achilles tendon ruptures can be successfully treated non-operatively, or operatively, but they must be treated. Surgical treatment leads to a faster recovery and a lower rate of re-rupture. However, surgery can be associated with very serious complications such as an infection or wound healing problems. For this reason non-operative treatment may be preferable in many individuals, especially those patients with diabetes, vascular disease, and those who are long-term smokers.Causes Causes of and contributors to Achilles tendon rupture include trauma (caused by injury, usually an acceleration injury such as pushing off or jumping up). Preceding tendon problems. Chronic Achilles tendonitis (can lead to small tears within the tendon, increasingly weakening it). Certain drug therapies/treatments. Drugs that have been linked to Achilles tendon rupture include. Fluoroquinolone antibiotics - after nearly 900 reports of tendon ruptures, tendonitis and other tendon disorders (most associated with the Achilles tendon) linked to Ciprofloxacin (Cipro) alone were collected in the U.S. Food and Drug Administration (FDA)s database, at least one public-interest group petitioned the FDA to recommend that a "Black Box Warning" be added to Cipro's packaging. Some researchers speculate this class of antibiotics is toxic to tendon fibers, and that in some cases may reduce their blood supply. Patients should at least be more aware of the potential for ruptures so that they can be switched to other antibiotics at the onset of early warning signals such as tendon pain. Symptoms Ankle pain and swelling or feeling like the ankle has given out after falling or stumbling. A loud audible pop when the ankle is injured. Patients may have a history of prior ankle pain or Achilles tendonitis, and may be active in sports. Swelling, tenderness and possible discoloration or ecchymosis in the Achilles tendon region. Indentation above the injured tendon where the torn tendon may be present. Difficulty moving around or walking. Individual has difficulty or is unable to move their ankle with full range of motion. MRI can confirm disruption or tear in the tendon. Inability to lift the toes. Diagnosis In diagnosing an Achilles tendon rupture, the foot and ankle surgeon will ask questions about how and when the injury occurred and whether the patient has previously injured the tendon or experienced similar symptoms. The surgeon will examine the foot and ankle, feeling for a defect in the tendon that suggests a tear. Range of motion and muscle strength will be evaluated and compared to the uninjured foot and ankle. If the Achilles tendon is ruptured, the patient will have less strength in pushing down (as on a gas pedal) and will have difficulty rising on the toes. The diagnosis of an Achilles tendon rupture is typically straightforward and can be made through this type of examination. In some cases, however, the surgeon may order an MRI or other advanced imaging tests. Non Surgical Treatment Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome.  Surgical Treatment Surgery will involve stitching the two ends of the tendon together, before placing the leg in a cast or brace. The advantage of having an operation is the reduced chance of the rupture reoccurring, however it will involve the risks associated with any surgical procedure, such as infection. Prevention Here are some suggestions to help to prevent this injury. Corticosteroid medication such as prednisolone, should be used carefully and the dose should be reduced if possible. But note that there are many conditions where corticosteroid medication is important or lifesaving. Quinolone antibiotics should be used carefully in people aged over 60 or who are taking steroids. |
Archives
July 2017
Categories |
 RSS Feed
RSS Feed
